10 mg/ml
For the use of a Registered Medical Practitioner or a Hospital or a Institution only.
PHENTOSOL (Phentolamine Mesilate) is an antihypertensive, for intravenous and intramuscular administration. Chemically Phentolamine Mesilate is 3-[[(4,5-Dihydro-1H-imidazol-2-yl)methyl](4-methylphenyl)amino]phenol methanesulfonate. Its molecular formula is C18H23N3O4S and molecular weight is 377.5.
STRUCTURAL FORMULA :
Its structural formula is :
-Structure.jpg)
PHENTOSOL is a clear colourless to pale yellow solution filled in amber glass ampoule of suitable size.
COMPOSITION :
Each ml contains :
Phentolamine Mesilate B.P. 10 mg
Anhydrous Glucose B.P. q.s.
Water for Injections B.P. q.s.
ACTIONS :
Phentolamine Mesilate produces an alpha-adrenergic block of relatively short duration. It also has direct, but less marked, positive inotropic and chronotropic effects on cardiac muscle and vasodilator effects on vascular smooth muscle.
PHARMACOKINETICS :
Following intravenous administration, the half-life of phentolamine has been reported to be 19 minutes. It is extensively metabolised and about 13 % of an intravenous dose is excreted unchanged in the urine.
INDICATIONS :
PHENTOSOL is indicated for the prevention or control of hypertensive episodes that may occur in a patient with pheochromocytoma as a result of stress or manipulation during preoperative preparation and surgical excision. PHENTOSOL is indicated for the prevention or treatment of dermal necrosis and sloughing following intravenous administration or extravasation of norepinephrine. PHENTOSOL is also indicated for the diagnosis of pheochromocytoma by the phentolamine blocking test.
For Intravenous and Intramuscular use only.
Pregnancy : Category C
There are no adequate and well-controlled studies in pregnant women. PHENTOSOL should be used during pregnancy only if the potential benefit justifies the potential risk to the foetus.
Nursing Mothers :
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from PHENTOSOL, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
INTERACTIONS :
Since phentolamine only blocks alpha-receptors, concomitant use of drugs such as adrenaline may lead to severe hypotension and tachycardia due to unopposed beta-adrenoreceptor stimulation.
SIDE EFFECTS :
The adverse effects of phentolamine are primarily due to its alpha-adrenoceptor blocking activity and include orthostatic hypotension and tachycardia. Myocardial infarction and cerebrovascular spasm or occlusion have been reported occasionally, usually in association with marked hypotension; flushing, sweating and feelings of apprehension may accompany hypotensive episodes. Anginal pain and arrhythmias have been reported rarely. Nausea, vomiting and diarrhoea may also occur. Other side effects include weakness, dizziness, flushing and nasal stuffiness.
OVERDOSAGE :
Acute Toxicity :
No deaths due to acute poisoning with phentolamine have been reported. Oral LD50s (mg/kg) : mice, 1000; rats, 1250.
Signs and Symptoms :
Overdosage with phentolamine is characterized chiefly by cardiovascular disturbances, such as arrhythmias, tachycardia, hypotension and possibly shock. In addition, the following might occur : excitation, headache, sweating, pupillary contraction, visual disturbances; nausea, vomiting, diarrhoea; hypoglycaemia.
TREATMENT OF OVERDOSAGE :
There is no specific antidote. A decrease in blood pressure to dangerous levels or other evidence of shock like conditions should be treated vigorously and promptly. The patients legs should be kept raised and a plasma expander should be administered. If necessary, intravenous infusion or norepinephrine, titrated to maintain blood pressure at the normotensive level and all available supportive measures should be included. Epinephrine should not be used, since it may cause a paradoxical reduction in blood pressure.
PHARMACEUTICAL PRECAUTIONS :
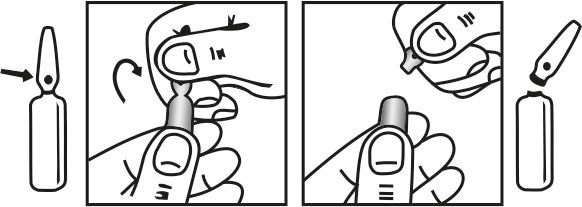
Product should be inspected visually for particulate matter and discoloration prior to administration. Discard the solution if it is discoloured or contain particulate matter.
STORAGE :
Store below 30°C (86°F), protected from light.
Do not refrigerate.
SHELF LIFE :
24 months from the date of manufacture.
PRESENTATION :
PHENTOSOL is supplied as 10 mg of Phentolamine Mesilate B.P. in 1 ml aqueous solution.
Such 3 ampoules of 1 ml are packed in a Box.
Disclaimer : For the use of a Registered Medical Practitioner or a Hospital or a Institution only. Also it is not intended to be used by healthcare professionals or patients for the purpose of prescribing or administering these products. Questions regarding the complete and current content of product labeling / specification / presentation should be directed to SGPharma.