




100 mg/ml, 250 mg/ml, 1 gm/10 ml
For the use of a Registered Medical Practitioner or a Hospital or a Institution only.
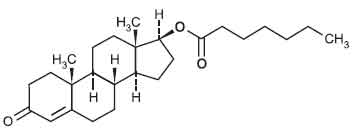
TESTOSTERONE ENANTHATE INJECTION USP (Testosterone Enanthate) is a derivative of the primary endogenous androgen testosterone. Chemically, Testosterone Enanthate is Androst-4-en-3-one, 17-(1-oxoheptyl)oxy-, (17β)-. The molecular formula is C26H40O3 and molecular weight is 400.59.
STRUCTURAL FORMULA :
Its structural formula is :
TESTOSTERONE ENANTHATE INJECTION USP is a sterile, pale yellow oily solution filled in amber ampoule of suitable size.
COMPOSITION :
Each ml contains :
Testosterone Enanthate USP 100 mg
Oily base q.s.
Contains no preservatives.
Each ml contains :
Testosterone Enanthate USP 200 mg
Oily base q.s.
Contains no preservatives.
Each ml contains :
Testosterone Enanthate USP 250 mg
Oily base q.s.
Contains no preservatives.
ACTIONS :
Endogenous androgens are responsible for the normal growth and development of the male sex organs and for maintenance of secondary sex characteristics. These effects include growth and maturation of prostate, seminal vesicles, penis, and scrotum; development of male hair distribution, such as beard, pubic, chest, and axillary hair; laryngeal enlargement; vocal chord thickening; alterations in body musculature; and fat distribution. Androgens also cause retention of nitrogen, sodium, potassium, and phosphorus, and decreased urinary excretion of calcium. Androgens have been reported to increase protein anabolism and decrease protein catabolism. Nitrogen balance is improved only when there is sufficient intake of calories and protein. Androgens are responsible for the growth spurt of adolescence and for the eventual termination of linear growth which is brought about by fusion of the epiphyseal growth centers. In children, exogenous androgens accelerate linear growth rates but may cause a disproportionate advancement in bone maturation. Use over long periods may result in fusion of the epiphyseal growth centers and termination of growth process. Androgens have been reported to stimulate the production of red blood cells by enhancing the production of erythropoietic stimulating factor. During exogenous administration of androgens, endogenous testosterone release is inhibited through feedback inhibition of pituitary luteinizing hormone (LH). At large doses of exogenous androgens, spermatogenesis may also be suppressed through feedback inhibition of pituitary follicle stimulating hormone (FSH). There is a lack of substantial evidence that androgens are effective in fractures, surgery, convalescence, and functional uterine bleeding.
PHARMACOKINETICS :
Absorption :
Testosterone esters are less polar than free testosterone. Testosterone esters in oil injected intramuscularly are absorbed slowly from the lipid phase; thus testosterone enanthate can be given at intervals of two to four weeks.
Distribution :
Testosterone in plasma is 98 % bound to a specific testosterone-estradiol binding globulin, and about two percent is free. Generally, the amount of this sex-hormone binding globulin in the plasma will determine the distribution of testosterone between free and bound forms, and the free testosterone concentration will determine its half-life.
Excretion :
About 90 % of a dose of testosterone is excreted in the urine as glucuronic and sulfuric acid conjugates of testosterone and its metabolites; about six percent of a dose is excreted in the faeces, mostly in the unconjugated form. Inactivation of testosterone occurs primarily in the liver. Testosterone is metabolized to various 17-keto steroids through two different pathways. The plasma half-life of testosterone is reported to range from about 10 to 100 minutes. In responsive tissues, the activity of testosterone appears to depend on reduction to dihydrotestosterone, which binds to cytosol receptor proteins. The steroid-receptor complex is transported to the nucleus where it initiates transcription events and cellular changes related to androgen action.
INDICATIONS :
Males :
TESTOSTERONE ENANTHATE INJECTION USP is indicated for replacement therapy in conditions associated with a deficiency or absence of endogenous testosterone.
Primary hypogonadism (congenital or acquired) :
Testicular failure due to cryptorchidism, bilateral torsion, orchitis, vanishing testis syndrome, or orchidectomy.
Hypogonadotropic hypogonadism (congenital or acquired) :
Idiopathic gonadotropin or luteinizing hormone-releasing hormone (LHRH) deficiency, or pituitary-hypothalamic injury from tumors, trauma, or radiation. (Appropriate adrenal cortical and thyroid hormone replacement therapy are still necessary, however, and are actually of primary importance.) If the above conditions occur prior to puberty, androgen replacement therapy will be needed during the adolescent years for development of secondary sexual characteristics. Prolonged androgen treatment will be required to maintain
sexual characteristics in these and other males who develop testosterone deficiency after puberty.
Delayed puberty :
TESTOSTERONE ENANTHATE INJECTION USP may be used to stimulate puberty in carefully selected males with clearly delayed puberty. These patients usually have a familial pattern of delayed puberty that is not secondary to a pathological disorder; puberty is expected to occur spontaneously at a relatively late date. Brief treatment with conservative doses may occasionally be justified in these patients if they do not respond to psychological support. The potential adverse effect on bone maturation should be discussed with the patient and parents prior to androgen administration. An X-ray of the hand and wrist to determine bone age should be obtained every six months to assess the effect of treatment on the epiphyseal center.
Females :
Metastatic mammary cancer :
TESTOSTERONE ENANTHATE INJECTION USP may be used secondarily in women with advancing inoperable metastatic (skeletal) mammary cancer who are one to five years postmenopausal. Primary goals of therapy in these women include ablation of the ovaries. Other methods of counteracting estrogen activity are adrenalectomy, hypophysectomy, and/or antiestrogen therapy. This treatment has also been used in premenopausal women with breast cancer who have benefited from oophorectomy and are considered to have a
hormone-responsive tumor. Judgment concerning androgen therapy should be made by an oncologist with expertise in this field.
Administration :
TESTOSTERONE ENANTHATE INJECTION USP is for I.M. use only. The injection must be administered extremely slowly. The oily solution is injected immediately after its drawing up into the syringe.
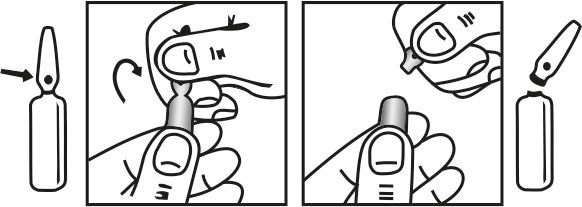
INSTRUCTIONS FOR USE OF AMPOULE :
The ampoule used in this product is equipped with O.P.C. (One Point Cut) opening system. No ampoule file is needed to open the ampoule. The neck of the ampoule is prescored at the point of constriction. A coloured dot on the ampoule head helps to orientate the ampoule. Take the ampoule and face the coloured dot. Let the solution at the head of the ampoule to flow down by shaking or a gentle stroke. The ampoule opens easily by placing the thumb on the coloured dot and gently pressing downwards as shown.
Dosage :
Dosage and duration of therapy with TESTOSTERONE ENANTHATE INJECTION USP will depend on age, sex, diagnosis, patient’s response to treatment, and appearance of adverse effects. When properly given, injections of TESTOSTERONE ENANTHATE INJECTION USP are well tolerated. Care should be taken to inject the preparation deeply into the gluteal muscle following the usual precautions for intramuscular administration. In general, total doses above 400 mg per month are not required because of the prolonged
action of the preparation. Injections more frequently than every two weeks are rarely indicated.
NOTE :
Use of a wet needle or wet syringe may cause the solution to become cloudy; however, this does not affect the potency of the material.
Male hypogonadism :
As replacement therapy, i.e., for eunuchism, the suggested dosage is 50 to 400 mg every 2 to 4 weeks.
In males with delayed puberty :
Various dosage regimens have been used; some call for lower dosages initially with gradual increases as puberty progresses, with or without a decrease in maintenance levels. Other regimens call for higher dosage to induce pubertal changes and lower dosage for maintenance after puberty. The chronological and skeletal ages must be taken into consideration, both in determining the initial dose and in adjusting the dose. Dosage is within the range of 50 to 200 mg every 2 to 4 weeks for a limited duration, for example, 4 to 6 months. X-rays should be taken at appropriate intervals to determine the amount of bone maturation and skeletal development.
Palliation of inoperable mammary cancer in women :
A dosage of 200 to 400 mg every 2 to 4 weeks is recommended. Women with metastatic breast carcinoma must be followed closely because androgen therapy occasionally appears to accelerate the disease.
Special populations
Children and adolescents :
TESTOSTERONE ENANTHATE INJECTION USP is not indicated for use in children and adolescents. Safety and efficacy have not been adequately determined in children and adolescents.
Elderly patients :
Limited data do not suggest the need for a dosage adjustment in elderly patients.
Patients with hepatic impairment :
No formal studies have been performed in patients with hepatic impairment. The use of TESTOSTERONE ENANTHATE INJECTION USP is contraindicated in men with past or present liver tumours.
Patients with renal impairment :
No formal studies have been performed in patients with renal impairment.
CONTRAINDICATIONS :
- Hypersensitivity to the active substance or to any of the excipients of the formulation.
- Androgen-dependent carcinoma of the prostate or of the male mammary gland.
- Hypercalcaemia.
- Past or present liver tumours.
- Nephrosis.
In patients with breast cancer and in immobilized patients, androgen therapy may cause hypercalcaemia by stimulating osteolysis. In patients with cancer, hypercalcaemia may indicate progression of bony metastasis. If hypercalcaemia occurs, the drug should be discontinued and appropriate measures instituted. Prolonged use of high doses of androgens has been associated with the development of peliosis hepatis and hepatic neoplasms including hepatocellular carcinoma. Peliosis hepatis can be a life-threatening or fatal complication. If cholestatic hepatitis with jaundice appears or if liver function tests become abnormal, the androgen should be discontinued and the etiology should be determined. Drug-induced jaundice is reversible when the medication is discontinued.
Geriatric patients treated with androgens may be at an increased risk for the development of prostatic hypertrophy and prostatic carcinoma. There have been postmarketing reports of venous thromboembolic events, including deep vein thrombosis (DVT) and pulmonary embolism (PE), in patients using testosterone products. Evaluate patients who report symptoms of pain, oedema, warmth and erythema in the lower extremity for DVT and those who present with acute shortness of breath for PE. If a venous thromboembolic event is suspected, discontinue treatment and initiate appropriate workup and management. Due to sodium and water retention, oedema with or without congestive heart failure may be a serious complication in patients with preexisting cardiac, renal, or hepatic disease. In addition to discontinuation of the drug, diuretic therapy may be required. If the administration of Testosterone Enanthate is restarted, a lower dose should be used. Gynaecomastia frequently develops and occasionally persists in patients being treated for hypogonadism.
Androgen therapy should be used cautiously in healthy males with delayed puberty. The effect on bone maturation should be monitored by assessing bone age of the wrist and hand every six months. In children, androgen treatment may accelerate bone maturation without producing compensatory gain in linear growth. This adverse effect may result in compromised adult stature. The younger the child the greater the risk of compromising final mature height.
PRECAUTIONS :
General :
Women should be observed for signs of virilization (deepening of the voice, hirsutism, acne, clitoromegaly, and menstrual irregularities). Discontinuation of drug therapy at the time of evidence of mild virilism is necessary to prevent irreversible virilization. Such virilization is usual following androgen use at high doses and is not prevented by concomitant use of estrogens. A decision may be made by the patient and the physician that some virilization will be tolerated during treatment for breast carcinoma. Because androgens may alter serum cholesterol concentration, caution should be used when administering these drugs to patients with a history of myocardial infarction or coronary artery disease. Serial determinations of serum cholesterol should be made and therapy adjusted accordingly. A causal relationship between myocardial infarction and hypercholesterolemia has not been established.
Pregnancy : Category X
Testosterone Enanthate is intended for use by men only. Testosterone Enanthate is not indicated in pregnant or breast feeding women. Testosterone Enanthate replacement therapy may reversibly reduce spermatogenesis.
Nursing mothers :
It is not known whether androgens are distributed into breast milk. Problems in humans have not been documented. However, androgens are rarely used by breast-feeding women and are not recommended. Potential adverse effects in infants include precocious sexual development in males and virilization of external genitalia in females.
Paediatric Use :
Androgens should be used with caution in children and adolescents who are still growing because of possible premature epiphyseal closure in males and females, precocious sexual development in prepubertal males, or virilization in females. Skeletal maturation should be monitored at 6-month intervals by an x-ray of the hand and wrist.
LABORATORY TESTS :
Women with disseminated breast carcinoma should have frequent determination of urine and serum calcium levels during the course of androgen therapy. Periodic (every six months) X-ray examinations of bone age should be made during treatment of pre-pubertal males to determine the rate of bone maturation and the effects of androgen therapy on the epiphyseal centers. Haemoglobin and haematocrit should be checked periodically for polycythaemia in patients who are receiving high doses of androgens.
INTERACTIONS AND INCOMPATIBILITIES :
Anticoagulants, coumarin- or indandione-derivative :
Anticoagulant effect may be increased because of decreased procoagulant factor concentration caused by alteration of procoagulant factor synthesis or catabolism and increased receptor affinity for the anticoagulant; anticoagulant dosage adjustment may be required during and following concurrent use.
Antidiabetic agents, sulfonylurea or Insulin :
Androgens may increase or decrease blood glucose; doses of insulin or antidiabetic sulfonylurea medications may need to be adjusted, especially if hypoglycaemia occurs.
Corticosteroids or Corticotropin :
Testosterone may contribute to the oedema that can occur with administration of corticotropin or corticosteroids; caution is recommended during concomitant administration in patients who have special risks, such as patients who have cardiac or hepatic disease.
Cyclosporine :
Methyltestosterone has been reported to increase plasma concentrations of cyclosporine and may increase the risk of nephrotoxicity; other androgens may have the same effect.
Hepatotoxic medications :
May result in an increased incidence of hepatotoxicity; patients should be carefully monitored, especially those undergoing long-term therapy or those with a history of liver disease.
Human growth hormone (somatrem or somatropin) :
Use of excessive doses of androgens in prepubertal males may accelerate epiphyseal maturation, although supplemental use of androgens may be necessary in patients with androgen deficiency to continue the growth response to human growth hormone.
Oxyphenbutazone :
Elevated serum levels of oxyphenbutazone may result.
SIDE EFFECTS :
Endocrine and Urogenital :
Female : The most common side effects of androgen therapy are amenorrhoea and other menstrual irregularities, inhibition of gonadotropin secretion, and virilization, including deepening of the voice and clitoral enlargement. The latter usually is not reversible after androgens are discontinued. When administered to a pregnant woman, androgens cause virilisation of the external genitalia of the female foetus. Male : Gynaecomastia, and excessive frequency and duration of penile erections. Oligospermia may occur at high dosages.
Skin and Appendages :
Hirsutism, male pattern baldness, and acne.
Fluid and Electrolyte Disturbances :
Retention of sodium, chloride, water, potassium, calcium, and inorganic phosphates.
Gastrointestinal :
Nausea, cholestatic jaundice, alterations in liver function tests; rarely, hepatocellular neoplasms, peliosis hepatis.
Haematologic :
Suppression of clotting factors II, V, VII, and X; bleeding in patients on concomitant anticoagulant therapy; polycythaemia.
Nervous System :
Increased or decreased libido, headache, anxiety, depression, and generalized paraesthesia.
Metabolic :
Increased serum cholesterol.
Miscellaneous :
Rarely, anaphylactoid reactions; inflammation and pain at injection site.
INFORMATION FOR PATIENTS :
Male adolescent patients receiving androgens for delayed puberty should have bone development checked every six months. The physician should instruct patients to report any of the following side effects of androgens :
Adult or adolescent males :
Too frequent or persistent erections of the penis.
Women :
Hoarseness, acne, changes in menstrual periods, or more facial hair.
All patients :
Any nausea, vomiting, changes in skin colour, or ankle swelling.
OVERDOSAGE AND TREATMENT OF OVERDOSAGE :
No special therapeutic measure apart from termination of therapy with the drug or dose reduction is necessary after overdosage. Acute toxicity data show that Testosterone Enanthate can be classified as non-toxic following a single intake. Even in the case of an inadvertent administration of a multiple of the dose required for therapy, no acute toxicity risk is expected.
PHARMACEUTICAL PRECAUTIONS :
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
STORAGE :
Store below 30°C (86°F), protected from light.
Do not refrigerate.
Warming and rotating the ampoule between the palms of the hands will redissolve any crystals that may have formed during storage at low temperatures.
SHELF LIFE :
24 months from the date of manufacture.
PRESENTATION :
TESTOSTERONE ENANTHATE INJECTION USP is supplied as per below table :
| Strength | Pack Size | Pack |
| 100 mg/ml | 1 ml Ampoule | Single Ampoule |
| 200 mg/ml | 1 ml Ampoule | Single Ampoule |
| 250 mg/ml | 1 ml Ampoule | Single Ampoule |
Disclaimer : For the use of a Registered Medical Practitioner or a Hospital or a Institution only. Also it is not intended to be used by healthcare professionals or patients for the purpose of prescribing or administering these products. Questions regarding the complete and current content of product labeling / specification / presentation should be directed to SGPharma.



