



25 mg/ml
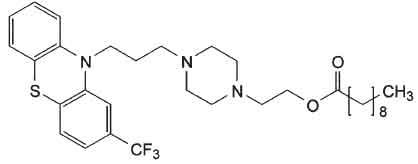
Fluphenazine Decanoate Injection USP (Fluphenazine Decanoate) is a phenothiazine with general properties similar to those of chlorpromazine. It has a piperazine side - chain. Fluphenazine is used in the treatment of variery of psychiatric disorders including schizophrenia, mania, Bipolar Disorder, severe anxiety, and behavioural disturbances. Chemically, Fluphenazine decanoate is 2-[4-[3-[2-(Trifluoromethyl)-10H-phenothiazin-10-yl]propyl]piperazin-1-yl]ethyl decanoate. The molecular formula is C32H44F3N3O2S and molecular weight is 591.8
STRUCTURAL FORMULA :
Its structural formula is :
Fluphenazine Decanoate Injection USP is a clear, light yellow oily liquid with little or no preceivable odour filled in ampoule of suitable size.
COMPOSITION :
Each ml contains :
Fluphenazine Decanoate USP 25 mg
Sesame Oil USP q.s.
ACTIONS :
Fluphenazine decanoate is an ester of the potent neuroleptic fuphenazine, a phenothiazine derivative of the piperazine type. The ester is slowly absorbed from the intramuscular site of injection and is then hydrolysed in the plasma to the active therapeutic agent, fluphenazine which then passes the blood brain barrier as the free drug. The mechanism of action of fluphenazine is attributed to dopamine receptor blockade in the mesolimbic system. It has weak anticholinergic effects, sedative effects, antiadrenal effects and neuroendocrine effects. Extrapyramidal reaction are common.
PHARMACOKINETICS :
Fluphenazine decanoate undergoes slow absorption from the site of intramuscular injection and is hydrolysed to release fluphenazine. Fluphenazine is extensively metabolised in the liver and excreted in the urine and faeces as unchanged drug and metabolites. Plasma level profiles of fluphenazine from Fluphenazine Decanoate Injection USP have shown half - lives of plasma clearance ranging from 2.5 to 16 weeks; this emphasises the importance of adjusting the dose and dose interval to the individual requirements of each patient. Because of the slow decline of plasma levels in most patients, a reasonably stable plasma level can usually be achieved with injections spaced at 2 to 4 week intervals.
INDICATIONS :
Fluphenazine decanoate is a long - acting antipsychotic agent. It is intended for use in the management of patients who require prolonged parenteral therapy with a neuroleptic drug, such as patients with schizophrenia and those with paranoid psychoses.
Administration :
Fluphenazine Decanoate Injection USP should be administered by deep intramuscular injection.
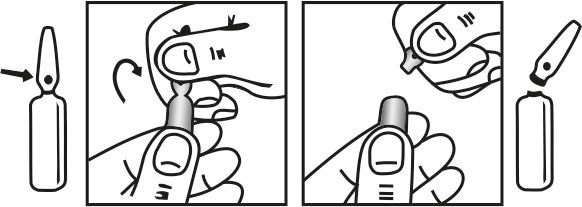
INSTRUCTIONS FOR USE OF AMPOULE :
The ampoule used in this product is equipped with O.P.C (One Point Cut) opening system. No ampoule file is needed to open the ampoule. The neck of the ampoule is prescored at the point of constriction. A coloured dot on the ampoule head helps to orientate the ampoule. Take the ampoule and face the coloured dot. Let the solution at the head of the ampoule to flow down by shaking or a gentle stroke. The ampoule opens easily by placing the thumb on the coloured dot and gently pressing downwards as shown.
Dosage :
Adults:
To begin therapy with fluphenazine decanoate the following regimens are suggested :
For most patients, a dose of 12.5 to 25 mg (0.5 to 1 ml) may be given to initiate therapy. The onset of action generally appears between 24 and 72 hours after injection and the effects of the drug on psychotic symptoms becomes significant within 48 to 96 hours. Subsequent injections and the dosage intervals are determined in accordance with the patient’s response. When administered as maintenance therapy, a single injection may be effective in controlling schizophrenic symptoms up to four weeks or longer. The response to a single dose has been found to last as long as six weeks in a few patients on maintenance therapy. It may be advisable that patients who have no history of taking phenothiazines should be treated initially with a shorter – acting form of fluphenazine before administering the decanoate to determine the patient’s response to fluphenazine and to established appropriate dosage. For psychotic patients who have been stabilized on a fixed daily dosage of fluphenazine hydrochloride tablets, fluphenazine hydrochloride elixir, or fluphenazine hydrochloride oral solution, conversion of therapy from these short - acting oral forms to the long - acting injectable fluphenazine decanoate may be indicated. Appropriate dosage of Fluphenazine Decanoate Injection USP should be individualized for each patient and responses carefully monitored. No precise formula can be given to convert to use of fluphenazine decanoate. However, a controlled multicentered study, in patients receiving oral doses from 5 to 60 mg fluphenazine hydrochloride daily, showed that 20 mg fluphenazine hydrochloride daily was equivalent to 25 mg (1ml) fluphenazine decanoate every three weeks. This represents an approximate conversion ration of 0.5 ml (12.5 mg) of decanoate every three weeks for every 10 mg of fluphenazine hydrochloride daily.
Once conversion to fluphenazine decanoate is made careful clinical monitoring of the patient and appropriate dosage adjustment should be made at the time of each injection. Severely agitated patients may be treated initially with a rapid - acting phenothiazine compound such as fluphenazine hydrochloride injection. When acute symptoms have subsided, 25 mg (1 ml) of fluphenazine decanoate may be administered; subsequent dosage is adjusted as necessary. “Poor risk” patients (those with known hypersensitivity to phenothiazines, or with disorders that predispose to undue reaction) : Therapy may be initiated cautiously with oral or parenteral fluphenazine hydrochloride, an equivalent dose of fluphenazine decanoate may be administered. Subsequent dosage adjustments are made in accordance with the response of the patient. The optimal amount of the drug and the frequency of administration must be determined for each patient, since dosage requirements have been found to vary with clinical circumstances as well as with individual response to the drug. Dosage should not exceed 100 mg. If doses greater than 50 mg are deemed necessary, the next dose and succeeding doses should be increased cautiously in increments of 12.5 mg.
Elderly :
The initial recommended dose or patients over 60 is 0.25 ml i.e. 6.25 mg. Elderly patients may be particularly susceptible to extrapyramidal reactions. Therefore a reduced maintenance dosage may be required.
Children :
Not recommended for children.
CONTRAINDICATIONS :
Phenothiazines are contraindicated in patients with suspected or established subcortical brain damage. Phenothiazine compounds should not be used in patients receiving large doses of hypnotics. Fluphenazine Decanoate Injection USP is contraindicated in comatose or severely depressed states. The presence of blood dyscrasia or liver damage precludes the use of fluphenazine decanoate. Fluphenazine docanoate is not intended for use in children under 12 years of age. Fluphenazine Decanoate Injection USP is contraindicated in patients who have shown hypersensitivity to fluphenazine; cross – sensitivity to phenothiazine derivatives may occur.
WARNINGS :
Fluphenazine Decanoate Injection USP contains benzyl alcohol as preservative. Benzyl alcohol has been reported to be associated with a fatal “Gasping Syndrome” in premature infants. Symptoms include a striking onset of gasping syndrome, hypotension, bradycardia and cardiovascular collapse.
Increased Mortality in Elderly Patients with Dementia - Related Psychosis :
Elderly patients with dementia – related psychosis treated with antipsychotic drugs are at an increased risk of death. Fluphenazine Decanoate Injection USP is not approved for the treatment of patients with dementia –related psychosis.
Tardive Dyskinesia :
Tardive dyskinesia, a syndrome consisting of potentially irreversible, involuntary, dyskinetic movements may develop in patients treated with neuroleptic (antipsychotic) drugs. Although the prevalence of the syndrome appears to be highest among the elderly, especially elderly women, it is impossible to rely upon prevalence estimates to predict, at the inception of neuroleptic treatment, which patients are likely to develop the syndrome. Whether neuroleptic drug products differ in their potential to cause tardive dyskinesia is unknown.
Both the risk of developing the syndrome and the likelihood that it will become irreversible are believed to increase as the duration of treatment and total cumulative dose of neuroleptic drugs administered to the patient increase. However, the syndrome can develop, although much less commonly, after relatively brief treatment periods at low doses.
There is no known treatment for established cases of tardive dyskinesia, although the syndrome may remit, partially or completely. If neuroleptic treatment is withdrawn. Neuroleptic treatment, itself, however, may suppress (or partially suppress) the sign and symptoms of the syndrome and thereby may possibility mask the underlying disease process. The effect that symptomatic suppression has upon the long – term course of the syndrome is unknown.
Given these considerations, neuroleptics should be prescribed in a manner that is most likely to minimize the occurrence of tardive dyskinesia. Chronic neuroleptic treatment should generally be reserved for patients who suffer from a chronic illness that,
1) is known to respond to neuroleptic drugs, and
2) for whom alternative, equally effective, but potentially less harmful treatments are not available or appropriate. In patients who do require chronic treatment, the smallest dose and the shortest duration of treatment producing a satisfactory clinical response should be sought. The need for continued treatment should be reassessed periodically.
If signs and symptoms of tardive dyskinesia appear in a patient on neuroleptics, drug discontinuation should be considered. However, some patients may require treatment despite the presence of the syndrome.
Neuroleptic Malignant Syndrome (NMS) :
A Potentially fatal symptom complex sometimes referred to as Neuroleptic Malignant Syndrome (NMS) has been reported in association with antipsychotic drugs. Clinical manifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis and cardiac dysrhythmias). The diagnostic evaluation of patients with this syndrome is complicated. In arriving at a diagnosis, it is important to identify cases where the clinical presentation includes both serious medical illness (e.g., pneumonia, systemic infection etc.) and untreated or inadequately treated extrapyramidal signs and symptoms (EPS). Other important considerations in the different diagnosis include central anticholinergic toxicity, heat stroke, drug fever and primary central nervous system (CNS) pathology.
The management of NMS should include :
1) Immediate discontinuation of antipsychotic drugs and other drugs not essential to concurrent therapy,
2) Intensive symptomatic treatment and medical monitoring and
3) Treatment of any concomitant serious medical problems for which specific treatments are available. There is no general agreement about specific pharmacological treatment regimens for uncomplicated NMS.
If a patient requires antipsychotic drug treatment after recovery from NMS, the potential reintroduction of drug therapy should be carefully considered. The patient should be carefully monitored. Since recurrence of NMS have been reported. The use of this drug may impair the mental and physical abilities required for driving a car or operating heavy machinery. Physicians should be alert to the possibility that severe adverse reactions may occur which require immediate medical attention. Potentiation of the effects of alcohol may occur with the use of this drug. Since there is no adequate experience in children who have received this drug, safety and efficacy in children have not been established.
PRECAUTION :
Leukopenia, Neutropenia and Agranulocytosis :
In clinical trial and postmarketing experience, events of leukopenia/neutropenia and agranulocytosis have been reported temporally related to antipsychotic agents. Possible risk factors for leukopenia/neutropenia include preexisting low white blood cell count (WBC) and history of drug induced leukopenia/neutropenia. Patients with a preexisting low WBC or history of drug induced leukopenia/neutropenia should have their complete blood count (CBC) monitored frequently during the first few months of therapy and should discontinue Fluphenazine Decanoate Injection USP at the first sign of a decline in WBC in the absence of other causative factors. Patients with neutropenia should be carefully monitored for fever or other symptoms or signs of infection and treated promptly if such symptoms or signs occur. Patients with severe neutropenia (absolute neutrophil count <1000/mm3) should discontinue Fluphenazine Decanoate injection USP and have their WBC followed until recovery.
General :
Because of the possibility of cross-sensitivity, fluphenazine decanoate should be used cautiously in patients who have developed cholestatic jaundice, dermatoses, or other allergic reactions to phenothiazine derivatives. Psychotic patients on large doses of a phenothiazine drug who are undergoing surgery should be watched carefully for possible hypotensive phenomena. Moreover, it should be remembered that reduced amounts of anaesthetics or central nervous system depressants may be necessary.
The effects of atropine may be potentiated in some patients receiving fluphenazine because of added anticholinergic effects.
Fluphenazine decanoate should be used cautiously in patients exposed to extreme heat or phosphorous insecticides.
The preparation should be used with caution in patients with a history of convulsive disorders, since grand mal convulsions have been known to occur.
Use with caution in patients with special medical disorders such as mitral insufficiency or other cardiovascular diseases and pheochromocytoma.
The possibility of liver damage, pigmentary retinopathy, lenticular and corneal deposits, and development of irreversible dyskinesia should be remembered when patients are on prolonged therapy. Outside state hospitals or other psychiatric institutions, fluphenazine decanoate should be administered under the direction of a physician experienced in the clinical use of psychotropic drugs, particularly phenothiazine derivatives. Furthermore, facilities should be available for periodic checking of hepatic function, renal function, and the blood picture. Renal function of patients on long-term therapy should be monitored; if BUN (blood urea nitrogen) becomes abnormal, treatment should be discontinued. As with any phenothiazine, the physician should be alert to the possible development of “silent pneumonias” in patients under treatment with fluphenazine decanoate.
Neuroleptic drugs elevate prolactin levels; the elevation persists during chronic administration. Tissue culture experiments indicate that approximately one-third of human breast cancers are prolactin dependent in vitro, a factor of potential importance if the prescription of these drugs is contemplated in a patient with a previously detected breast cancer. Although disturbances such as galactorrhea, amenorrhea, gynecomastia, and impotence have been reported, the clinical significance of elevated serum prolactin levels is unknown for most patients. An increase in mammary neoplasms has been found in rodents after chronic administration of neuroleptic drugs. Neither clinical studies nor epidemiologic studies conducted to date, however, have shown an association between chronic administration of these drugs and mammary tumorigenesis; the available evidence is considered too limited to be conclusive at this time.
Information to patients :
Given the likelihood that some patients exposed chronically to neuroleptics will develop tardive dyskinesia, it is advised that all patients in whom chronic use is contemplated be given, if possible, full information about this risk. The decision to inform patients and/or their guardians must obviously take into account the clinical circumstances and the competency of the patient to understand the information provided.
Pregnancy :
The safety for the use of this drug during pregnancy has not been established; therefore, the possible hazards should be weighed against the potential benefits when administering this drug to pregnant patients.
Nursing mothers :
Breast feeding should be avoided because of the possibility that fluphenazine is excreted in breast milk.
Paediatric Use :
Not recommended for children.
INTERACTIONS :
The possibility should be borne in mind that phenothiazines may :
Increase the CNS - depressant effects of drugs such as alcohol, general anaesthetics, hypnotics, sedatives or strong analgesics. Antagonise the action of sympathomimetic agents, including adrenaline and reverse the blood - pressure lowering effects of adrenergic - blocking agents such as guanethidine and clonidine. Impair the anti - parkinsonian effect of L - dopa, the effect of anticonvulsants, the metabolism of tricyclic antidepressants and the control of diabetes mellitus. Increase the effect of anticoagulants and antidepressants.
Interact with lithium.
Enhance the anticholinergic effects of other anticholinergic drugs, including the antimuscarinic anti - parkinsonian agents. Phenothiazines may also enhance the cardiac depressant effects of quinidine, the absorption of corticosteroids and digoxin and of neuromuscular blocking agents.
SIDE EFFECTS :
Central Nervous System :
The side effects most frequently reported with phenothiazine compounds are extrapyramidal symptoms including pseudoparkinsonism, dystonia, dyskinesia, akathisia, oculogyric crises, opisthotonos, and hyperreflexia. Muscle rigidity sometimes accompanied by hyperthermia has been reported following use of fluphenazine decanoate. Most often these extrapyramidal symptoms are reversible, however, they may be persistent. The frequency of such reactions is related in part to chemical structure : one can expect a higher incidence with fluphenazine decanoate than with less potent piperazine derivatives or with straight-chain phenothiazines such as chlorpromazine. With any given phenothiazine derivative, the incidence and severity of such reactions depend more on individual patient sensitivity than on other factors, but dosage level and patient age are also determinants.
Extrapyramidal reactions may be alarming, and the patient should be forewarned and reassured. These reactions can usually be controlled by administration of antiparkinsonian drugs such as Benztropine Mesylate or intravenous Caffeine and Sodium Benzoate Injection, and by subsequent reduction in dosage.
Dystonia :
Class effect : Symptoms of dystonia, prolonged abnormal contractions of muscle groups, may occur in susceptible individuals during the first few days of treatment. Dystonic symptoms include : spasm of the neck muscles, sometimes progressing to tightness of the throat, swallowing difficulty, difficulty breathing, and/or protrusion of the tongue. While these symptoms can occur at low doses, they occur more frequently and with greater severity with high potency and at higher doses of first generation antipsychotic drugs. An elevated risk of acute dystonia is observed in males and younger age groups.
Tardive Dyskinesia :
See WARNINGS. The syndrome is characterized by involuntary choreoathetoid movements which variously involve the tongue, face, mouth, lips, or jaw (e.g., protrusion of the tongue, puffing of the cheeks, puckering of the mouth, chewing movements), trunk and extremities. The severity of the syndrome and the degree of impairment produced vary widely. The syndrome may become clinically recognizable either during treatment, upon dosage reduction, or upon withdrawal of treatment. Early detection of tardive dyskinesia is important. To increase the likelihood of detecting the syndrome at the earliest possible time, the dosage of neuroleptic drug should be reduced periodically (if clinically possible) and the patient observed for signs of the disorder. This maneuver is critical, since neuroleptic drugs may mask the signs of the syndrome.
Other CNS Effects :
Occurrences of neuroleptic malignant syndrome (NMS) have been reported in patients on neuroleptic therapy; leukocytosis, elevated CPK, liver function abnormalities, and acute renal failure may also occur with NMS. Drowsiness or lethargy, if they occur, may necessitate a reduction in dosage; the induction of a catatonic-like state has been known to occur with dosages of fluphenazine far in excess of the recommended amounts. As with other phenothiazine compounds, reactivation or aggravation of psychotic processes may be encountered. Phenothiazine derivatives have been known to cause, in some patients, restlessness, excitement, or bizarre dreams.
Autonomic Nervous System :
Hypertension and fluctuations in blood pressure have been reported with fluphenazine. Hypotension has rarely presented a problem with fluphenazine. However, patients with pheochromocytoma, cerebral vascular or renal insufficiency, or a severe cardiac reserve deficiency such as mitral insufficiency appear to be particularly prone to hypotensive reactions with phenothiazine compounds, and should therefore be observed closely when the drug is administered. If severe hypotension should occur, supportive measures including the use of intravenous vasopressor drugs should be instituted immediately. Levarterenol Bitartrate Injection is the most suitable drug for this purpose; epinephrine should not be used since phenothiazine derivatives have been found to reverse its action, resulting in a further lowering of blood pressure. Autonomic reactions including nausea and loss of appetite, salivation, polyuria, perspiration, dry mouth, headache, and constipation may occur. Autonomic effects can usually be controlled by reducing or temporarily discontinuing dosage. In some patients, phenothiazine derivatives have caused blurred vision, glaucoma, bladder paralysis, faecal impaction, paralytic ileus, tachycardia, or nasal congestion.
Metabolic and Endocrine :
Weight change, peripheral oedema, abnormal lactation, gynaecomastia, menstrual irregularities, false results on pregnancy tests, impotency in men and increased libido in women have all been known to occur in some patients on phenothiazine therapy.
Allergic Reactions :
Skin disorders such as itching, erythema, urticaria, seborrhea, photosensitivity, eczema and even exfoliative dermatitis have been reported with phenothiazine derivatives. The possibility of anaphylactoid reactions occurring in some patients should be borne in mind.
Haematologic :
Routine blood counts are advisable during therapy since blood dyscrasias including leukopenia, agranulocytosis, thrombocytopenic or nonthrombocytopenic purpura, eosinophilia, and pancytopenia have been observed with phenothiazine derivatives. Furthermore, if any soreness of the mouth, gums, or throat, or any symptoms of upper respiratory infection occur and confirmatory leukocyte count indicates cellular depression, therapy should be discontinued and other appropriate measures instituted immediately.
Hepatic :
Liver damage as manifested by cholestatic jaundice may be encountered, particularly during the first months of therapy; treatment should be discontinued if this occurs. An increase in cephalin flocculation, sometimes accompanied by alterations in other liver function tests, has been reported in patients receiving the enanthate ester of fluphenazine (a closely related compound) who have had no clinical evidence of liver damage.
Others :
Sudden, unexpected and unexplained deaths have been reported in hospitalized psychotic patients receiving phenothiazines. Previous brain damage or seizures may be predisposing factors; high doses should be avoided in known seizure patients. Several patients have shown sudden flare-ups of psychotic behavior patterns shortly before death. Autopsy findings have usually revealed acute fulminating pneumonia or pneumonitis, aspiration of gastric contents, or intramyocardial lesions. Although this is not a general feature of fluphenazine, potentiation of central nervous system depressants (opiates, analgesics, antihistamines, barbiturates, alcohol) may occur. The following adverse reactions have also occurred with phenothiazine derivatives; systemic lupus erythematosus-like syndrome, hypotension severe enough to cause fatal cardiac arrest, altered electrocardiographic and electroencephalographic tracings, altered cerebrospinal fluid proteins, cerebral edema, asthma, laryngeal edema, and angioneurotic edema; with long-term use - skin pigmentation, and lenticular and corneal opacities. Injections of fluphenazine decanoate are extremely well tolerated, local tissue reactions occurring only rarely.
OVERDOSAGE AND TREATMENT OF OVERDOSAGE :
The expected symptoms of overdosage would be an exaggeration of the known pharmacological effects of fluphenazine and might therefore include extrapyramidal reactions, hypotension and excessive sedation. There is no specific antidote to fluphenazine and treatment of overdose is symptomatic and supportive. Severe extra - pyramidal reactions should be treated with an antiparkinsonian agent. Severe hypotension may be managed by placing the patient in the head - down position and, if necessary, administering plasma expanders. If a vasoconstrictor is required, metaraminol or noradrenaline should be used; adrenaline should be avoided as it may further lower the blood pressure through interaction with the phenothiazine. A patent airway should be established and respiratory depression may be managed by artificial respiration. Treatment of overdose is symptomatic and supportive. Severe extra - pyramidal reactions should be treated with an antiparkinsonian agent.
PHARMACEUTICAL PRECAUTIONS :
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
STORAGE :
Store below 30°C (86°F), protected from light.
Do not refrigerate.
SHELF LIFE :
24 months from the date of manufacture.
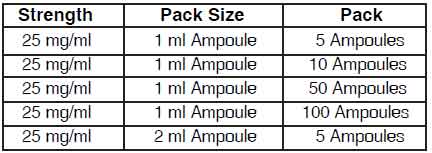
PRESENTATION :
Fluphenazine Decanoate Injection USP is supplied as per below table:
For the use of a Registered Medical Practitioner or a Hospital or a Institution only.






